It seems as if the slogan of our policy makers and planners is: surrender your natural resources- we shall give you an undernourished, ailing, unequal development in return.They cause a tradeoff between resources and a corrupt, unaccountable bunch of schemes: 5 kg grains per head, a meal for Rs. 5 students in schools, a nutritious meal for Rs. 6 at Aanganwadis; a grist of a healthy, well-nourished childhood policy. Now the moot question is: how can we expect a panacea from the policies and the perspective that gave a free ride to malnutrition and sickness to invade the innards of our children? A nation of 55 million sick children cannot be cured with rickety schemes. It calls for an overhaul of basic priorities.
Take the case of 3 year old Shubham of Dulhaniyapur village in district Kaushambi of UP. Being the seventh child of his family, Shubham did not receive proper care early on. By the age of 6 months, he should have received external/adjunct nutrition, but for 2 years lived solely on his mother’s milk. Presently, he is severely under-nourished.
In Dulhaniyapur, the mother’s first milk, colostrum, is considered harmful, even today! 9 out of ten girls of the village suffer from anemia. Parasite infestation has resulted in bloated bellies. Symptoms of hepatomegaly, a condition of an enlarged liver, are also found in malnourished children. Aanganwadi centres do not open or function. Growth charts are accumulating dust. Expired medicines, scattered dirty sacks of nutrients/nutritional foods are the telltale signs of the grim reality of the (mal) nutritional status of our children. Except
This sorry tale continues in the Upari Khori village of the Sahariya-dominated district of Sheopur in MP. Three out of 5 children are malnourished while every fourth child of the village is severely undernourished. Satnam, A malnourished child was not able to reach the local Nutritional Rehabilitation Nutrition Centre in time. He died on 15th October, 2015. Four year old Saroj of Tiktoli village was also a victim of the same fate. Severely malnourished Saroj could not be taken in time to the nearest nutrition rehabilitation centre, and she died on 30th September, 2015. The Aanganwadi of Tiktoli has remained shut for the last year.
All the discussions about this abominable state of affairs boils down to the level of Anganwadis meant for providing nutrition to children. Actually, to deal with this situation, it is imperative to grapple with the issues of food (in) security and lack of mother’s care in early childhood. Add into this the restoration and assertion of women’s autonomy in the matters pertaining to their social-economic-political status and decision making. It cannot be left or reduced to one department or one scheme only. Pro-active inbuilt inter-sectoral convergence system among health, nutrition, livelihoods, right to safe drinking water and education should be the key governance priority at the “state” functions. Having said that, community based management of malnutrition by giving equal space to the issues of agriculture, land, social-equality and community’s rights over natural resources is the only way forward. There is an urgent need of improving the food habits by de-recognizing the importance of packaged food and give priority to locally available and culturally acceptable food; at both the levels of family and in government run nutrition programs. It will be a disastrous to give entry to packaged and pre-cooked food, as on one hand, it will exclude the community from the governance of such programs forever and on the other hand it will become an ultimate threat to the community-centric food security mechanisms.
 Dr. Vandana Prasad (Ex-Member of National Commission for the Protection of Child Rights, Government of India) says we need to focus on community-based management of malnutrition and access to qualitative health services. Our children do not require miracles; they just need oil, eggs, fruit, vegetables and safe drinking water in their diet plus a policy focus for providing the rights to livelihood and natural resources.he only way forward. There is an urgent need of improving the food habits by de-recognizing the importance of packaged food and give priority to locally available and culturally acceptable food; at both the levels of family and in government run nutrition programs. It will be a disastrous to give entry to packaged and pre-cooked food, as on one hand, it will exclude the community from the governance of such programs forever and on the other hand it will become an ultimate threat to the community-centric food security mechanisms.
Dr. Vandana Prasad (Ex-Member of National Commission for the Protection of Child Rights, Government of India) says we need to focus on community-based management of malnutrition and access to qualitative health services. Our children do not require miracles; they just need oil, eggs, fruit, vegetables and safe drinking water in their diet plus a policy focus for providing the rights to livelihood and natural resources.he only way forward. There is an urgent need of improving the food habits by de-recognizing the importance of packaged food and give priority to locally available and culturally acceptable food; at both the levels of family and in government run nutrition programs. It will be a disastrous to give entry to packaged and pre-cooked food, as on one hand, it will exclude the community from the governance of such programs forever and on the other hand it will become an ultimate threat to the community-centric food security mechanisms.
Biraj Patnaik (Member of the Working Group for Children under 6 Yrs.) adds “The Supreme Court has passed more than ten important orders, under the provisions of ICDS. But bypassing these orders, very limited provisions have been made for the nutritional rights of our children in the National Food Security Act. In fact, a blueprint should be made part of the Food Security Act. It should contain a qualitative, universal and independent accountability mechanism of ICDS and a community-based management of malnutrition.
According to Ms. Deepika Sharma of UNICEF, frequent illness and non-availability of proper and adequate nutritious food is the immediate cause of malnutrition in children. Now is the time for us to ensure the right of safe, potable water along with eradicating the root, underlying causes of malnutrition. These causes are child marriage, child labour, caste and gender based discrimination, landlessness, lack of livelihood security, and climate change. Without attacking all these problems, we cannot rid our country of malnutrition.
Stunted Childhood
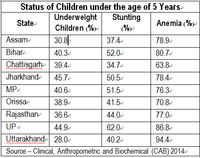 In UP, 62%; in Bihar, 52%; in MP, 51.5% and in Jharkhand 50.5% of children in the age group 5-59 months are in the grip of stunting malnutrition.
In UP, 62%; in Bihar, 52%; in MP, 51.5% and in Jharkhand 50.5% of children in the age group 5-59 months are in the grip of stunting malnutrition.
In a Clinical, Anthropometric and Biochemical (CAB – 2014) evaluation of 9 backward states of the country, especially with respect to the nutritional status of children, the fact that came up is more than half of our children suffer from stunted height, weight growth in their respective age group. The occurrence of this kind of malnutrition is not a sudden phenomenon. Inadequate mother’s milk in the first six months of a newborn baby’s life is manifested in growth-hampering malnutrition. A contributing factor is also a lack of proper child care, health services and assorted food items which in the latter period create a crisis situation. NSSO data point towards a consistently decreasing consumption of protein in the country.
If we take state-wise monthly consumption (of Pulses) per head in rural areas as a yardstick, against the national consumption of 783 gm-MP gets 850 gm, Bihar gets 740 gm, Jharkhand consumes 477 gm, UP consumes 860 gm, and Rajasthan receives 570 gm of dal (Pulses) in their respective thalis (Food Plate). To deal with malnutrition, Fat too is a necessary ingredient in our diets. In rural MP, a person consumes 640 gm fat monthly, in UP this figure is 840 gm, in Rajasthan it’s 650 gm, in Bihar 580 gm, in Chhattisgarh the figure is 600 gm, and at the all-India level, monthly consumption per head of fat is 674 gm. Monthly, per person consumption of grain at the national level is 11.800 kg. (333 gm daily), which is sub-standard.
Threats of Anemia
Like malnutrition, the scourge of anemia, too, has reached a nadir. But, while presenting the GDP data, this indicator is kept hidden. In Uttarakhand, 94.4% of under 5 year age children suffer from anemia, whereas for UP this figure is 86.8 per cent, for Bihar it’s 80.7%, in Assam this percentage is 78.9, and in Jharkhand 78.4% of under 5 children are suffering from anemia. As a result, their growth is impacted, hampered-they tire very easily, and their concentration levels are quite low.
The scourge of malnutrition cannot be eradicated until: our adolescent girls/daughters are treated well and at par, every woman gets her right of motherhood, child-feeding practices are corrected properly, safe and clean drinking is made available, and a decentralized, diversified production pattern gets established. Our problem of malnutrition has not been posited properly in our overall politico-socio-economic discourse. According to Rapid Survey on Children, only 44.6% of children (age: 0-23 months) in India were fortunate to receive their mother’s milk in the first hours of their life. And only 50.5% of our children (age: 6-8 months) receive additional/external food. It means, children are ‘kept’ hungry, trapping them in the vicious circle of malnutrition-illness-poverty.
Status of Adolescent Girls
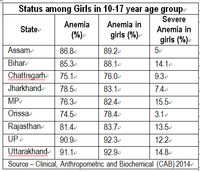 It is essential to understand the human life cycle in order to break the nexus of malnutrition, IMR, MMR and poverty. It is forbidden for adolescent girls in the family to talk about hormonal, psychosomatic and physical changes which are natural at their age. According to CAB-2014, in Uttarakhand 92.9% of the girls in the age group 10-17 suffer from anemia; for UP, this figure is 92.3%; for Assam, its 89.2%, for Bihar, it is 88.1 and in MP, 82.4 per cent of the girls in this age group are suffering from anemia. In MP, 15.5%; in Uttarakhand, 14.8% and in Bihar, 14.1% girls are the victims of severe anemia. This condition has direct and adverse implications for MMR, low birth weight, IMR, and risk of serious illnesses.
It is essential to understand the human life cycle in order to break the nexus of malnutrition, IMR, MMR and poverty. It is forbidden for adolescent girls in the family to talk about hormonal, psychosomatic and physical changes which are natural at their age. According to CAB-2014, in Uttarakhand 92.9% of the girls in the age group 10-17 suffer from anemia; for UP, this figure is 92.3%; for Assam, its 89.2%, for Bihar, it is 88.1 and in MP, 82.4 per cent of the girls in this age group are suffering from anemia. In MP, 15.5%; in Uttarakhand, 14.8% and in Bihar, 14.1% girls are the victims of severe anemia. This condition has direct and adverse implications for MMR, low birth weight, IMR, and risk of serious illnesses.
According to Rapid Survey on Children (Commissioned by the Department of Women and Child Welfare; 20143-14) 44.7% adolescent girls are weak and malnourished; and in many parts of the scourge of child marriages continues.
• The number of girls under 19 is 234.5 Million in India, of which n15 millon are married (5.6%).
• 3.8 Million of these girls had become mothers (29%). Doesn’t this fact prove the harsh/ bitter reality that reproduction becomes an obligation for any girl/woman after marriage? This kind of situation is the biggest risk to the lives of every female.
• These under 19 married-girls had given birth to 6.014 Million children.
• By their 19th year, 926 Thousand girls had become the mothers of 2 children.
• In the 15-19 year age group there were 56.5 Million girls in India, of which 11.2 Million were married.
• Out of these 11.2 Million married girls, 3.35 Million girls had already become mothers.
The Ground Reality of Packaged Food Items
Of 5 children of Rekha nat (name changed) of Dulhaniyapur village, Rehan is three months old. His weight at birth was 2.800 kg. Presently, Rehan is suffering from severe malnutrition. Azem Bhai, the father-in-law of Rekha, says that his monthly bill for baby food is Rs. 385. Despite such a dire poverty situation, how can one remain insensitive to their children! In a study done in MP and UP (Vikas Samvad; 2013-15) it was found that 93% of village kirana shops are selling 19 kinds of packaged food items (Puffs, Peas, Kurmure). In this study it was found that some 11-19 thousand packets of such food items, priced between Rs. 1 to Rs. 5 are being sold annually in a typical village of 250 houses. One such retailer, Mohd. Idris says, “Being pre-cooked or already processed, these food items do not require any cooking at home; children like them, and once consumed, they retain their flavor and taste on the taste buds of the consumer.” But these food items are nothing but junk. They do not fulfill the nutritional needs of our children. In fact, we are creating a big crisis in the name of economic development.
According to Unicef nutrition specialist, Ms. Deepika Sharma, “…Stunting has clear linkages with poor child development and stunting before the age of 2 years leads to lower cognitive ability and educational outcomes in later childhood and adolescence. Primarily, the key causes of stunting are inadequate nutrition and frequent infection. In most cases it begins in the womb and the damage done in the first two years of life is largely irreversible. Therefore, focusing on the critical 1000-day window from a woman’s pregnancy to her child’s second birthday is of utmost importance.
However, the underlying and root causes shape the delivery and implementation of nutrition information and services. Underlying factors such as situations of food insecurity, inadequate care-giving practices, women’s autonomy and decision making, as well as environmental conditions impact the health and nutrition status of a child. To address the issue we need consistent and quality implementation of flagships schemes and other programs addressing malnutrition, functional convergence among key departments and community groups. Differential programming for the most marginalized communities is needed to address the challenge. Nutrition is a multi-dimensional issue and demands a multi-sector response.
Nutritional Crisis is a multi-dimensional challenge and cannot be dealt with by limiting it to Integrated Child Development Services and its Supplementary Nutrition Program. Recent findings by Clinical, Anthropometric and Biochemical (CAB – 2014) evaluation report clearly shows that, on the one hand communities are living in chronic poverty and on the other hand changing food habits are becoming new challenges. Does it mean that economic growth is taking responsible food behavior away?
# # #
About the Author- Mr. Sachin Kumar Jain is a development journalist and researcher who is associated with the Right to Food Campaign in India and works with Vikas Samvad, AHRC’s partner organisation in Bhopal, Madhya Pradesh. He could be contacted at sachin.vikassamvad@gmail.com